Note added 10/11/21: The microchemistry evidence in favour of Ivermectin now looks definitive. In particular it looks like Ivermectin is at least as effective, and probably more effective, than the new Pfizer anti-viral. The main difference is that Ivermectin is virtually free, whereas Pfizer will be charging the earth for their new drug. Watch this video: https://www.youtube.com/watch?v=ufy2AweXRkc
*********************
Apologies for this off-topic post, but I’ll make it brief.
I have carried out an independent literature review of the efficacy of Ivermectin in prophylaxis or treatment of Covid-19. I thought, having done it, I might as well make it more widely available. It is here.
The conclusion is that the balance of evidence is in favour of efficacy, and that Ivermectin is a safe drug. Claims that abound from Google searches that excessive doses are required for clinical efficacy are simply false.
As of their last report (March 2021), the World Health Organisation continues to recommend NOT using Ivermectin against Covid-19, except in the context of clinical trials. The conclusions from their own meta-analysis are strangely at odds with what I found in the literature.
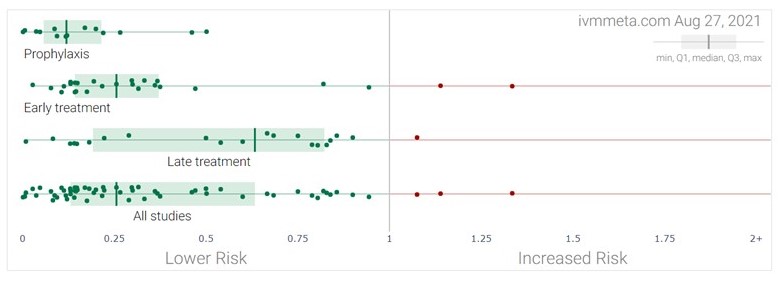
I found many papers calling for large scale trials, going back to early in the pandemic. But the funding necessary for large trials, which would have to come from national or international authorities, or from Big Pharma, did not materialise and so neither did the large scale trials. Instead we have many small trials, funded locally by individual research centres or hospitals. In this situation, when conducting meta-analyses, it becomes necessary to include studies which might normally be rejected – otherwise the situation becomes a self-fulfilling impasse in which lack of big funding means lack of big trials means “no statistically significant evidence”. But the statistical significance arises only when many small trials are aggregated.