[Added 26/7/17: Here is an example of why men absolutely need an effective contraceptive]
Male contraception is a bit like fusion power: it’s just a few years away and has been for over half a century. Is male contraception truly now just a few years away? Here I review the state-of-play, starting with the brief excitement last October.
Hormonal Drug Methods
There was much ado last October (2016) with the publication of the ‘latest’ study (Efficacy and Safety of an Injectable Combination Hormonal Contraceptive for Men, Hermann Behre et al in The Journal of Clinical Endocrinology & Metabolism, Vol.101, Issue 12 – the full article may be downloaded from here). What the many reports did not bother to mention was that the clinical trials upon which this report was based, which started in September 2008, were completed by May 2012, some four and a half years prior to the publication. In fact, the last injection was carried out in March 2011, five and a half years prior to the publication. So this ‘latest’ study is hardly very recent, and one wonders why it took so very long to publish the findings.
There is no mystery, however, regarding the premature termination of the Behre et al trials. All such clinic trials are subject to approval and monitoring by ethics committees. To quote the paper,
“An independent Data Safety and Monitoring Committee (DSMC) was established by WHO/RHR and CONRAD before the start of the trial. At the scheduled meeting on January 17, 2011, the committee reviewed the interim analysis data and determined the study met all criteria for continuation.”
where, WHO/RHR is the World Health Organization, Department of Reproductive Health and Research, and CONRAD is a cooperative agreement between Eastern Virginia Medical School and the U. S. Agency for International Development, these being the funding bodies, together with grants from the Bill & Melinda Gates Foundation.
So, in January 2011 everything seemed fine to continue the trials. But…
“As part of WHO/RHR’s continuing monitoring review of all its ongoing studies, the department’s Research Project Review Panel, an external peer-review committee, met in March 2011, reviewed the same data and determined that, for safety reasons, recruitment should be stopped and enrolled participants should discontinue receiving injections and be transitioned to the recovery phase.”
Having become rather jaundiced about our medical ethics community, I do wonder who sits on this external peer-review committee. However, the report notes,
“This decision was based on the Review Panel’s study of the Adverse Events and the conclusion that the risks to the study participants outweighed the potential benefits to the study participants and to the increased precision of the study outcome findings from having the full cohort contribute to the final analysis.”
Certainly there were adverse outcomes. After screening for being initially sufficiently fertile, and other measures of good health, 320 couples started the trials. Adverse outcomes were summarised as follows,
“There was 1 death by suicide in the efficacy phase that was assessed as not related to the study regimen. The participant received 3 injections and committed suicide 1 month after the last injection. The family indicated that he could not cope with his academic pressure. Other nonfatal serious adverse events were 1 case of depression (assessed as probably related) and 1 case of intentional paracetamol over-dose (assessed as possibly related) during the suppression phase, as well as 1 case of tachycardia with paroxysmal atrial fibrillation (assessed as possibly related) during the recovery phase. Ten other serious adverse events were assessed as not being related to the study regimen.
Twenty men discontinued the study due to product-related side effects. Of these 20, 6 men discontinued only for changes in mood, and 6 men discontinued for the following single reasons: acne, pain or panic at first injection, palpitations, hypertension, and erectile dysfunction. Eight men discontinued for more than 1 side effect, including multiple reasons related to changes in mood.”
Media reports of the Behre et al study delighted in claiming that the trials had been discontinued because “men can’t handle side effects women face daily“. The sub-text here is that women, it seems, are very desirous of men taking over responsibility for contraception. And, as Samantha Allen put it, there’s strong evidence that men are willing to shoulder some side effects to get more involved in contraception. Well, that makes a change from women’s usual rejoinder that “you couldn’t trust a man to take responsibility for contraception”.
What these popular reports seem not to recognise is the potentially game-changing nature of effective male contraception. The Pill was instrumental in liberating women from the occupational hazard of pregnancy. It allowed women easily to take effective control of their fertility. Men currently have little control of their fertility, especially if they are relying on their partner to deal with it. Certain feminists are well aware of this imbalance and like it that way. It’s all about power with such feminists. So if there is an increasing mood among women in favour of male contraception, that’s a welcome development.
It’s been known since at least 1990 that testosterone has a “contraceptive efficacy comparable with modern female methods” (Behre et al). This was demonstrated by a large study of over 1000 Chinese men reported in 2011 but the Chinese company involved never followed up with further testing or by seeking regulatory approval. In any case, the large doses of testosterone required would probably have long-term adverse health effects. The testosterone dose can be reduced by coadministration of a progestogen. The Behre et al trials were for the purpose of testing this combined drug treatment. The trials involved an injection every eight weeks. The average sperm count was 55 million/mL prior to injection, and 95% of men became functionally infertile with a sperm count not exceeding 1 million/mL by week 24. Yes, it does take that long, as shown by Figure 1 below – which is not terribly convenient, is it?
Figure 1 (Suppression of 1 defined as sperm count <1 million/mL) – click to enlarge

However, I think the graph is misleading. Sperm counts were taken at the same time that injections were administered. Consequently the effects of the first injection would not be measured for eight weeks. Arguably, the whole of the above graph should be shifted to the left by eight weeks – so that 95% confidence in contraception would be achieved in 16 weeks – still not exactly quick. But, on this interpretation, 80% confidence would be achieved in just eight weeks – rather better.
Four women became pregnant despite the men having sperm counts less than 1 million/mL, a failure rate of 1.5%. However, all four occurred during the first 16 weeks of the ‘efficacy phase’, none thereafter. [Without wishing to cast aspersions, there was no check that the men in the trial were responsible for these pregnancies, and 1.5% is well within expected mis-paternity rates].
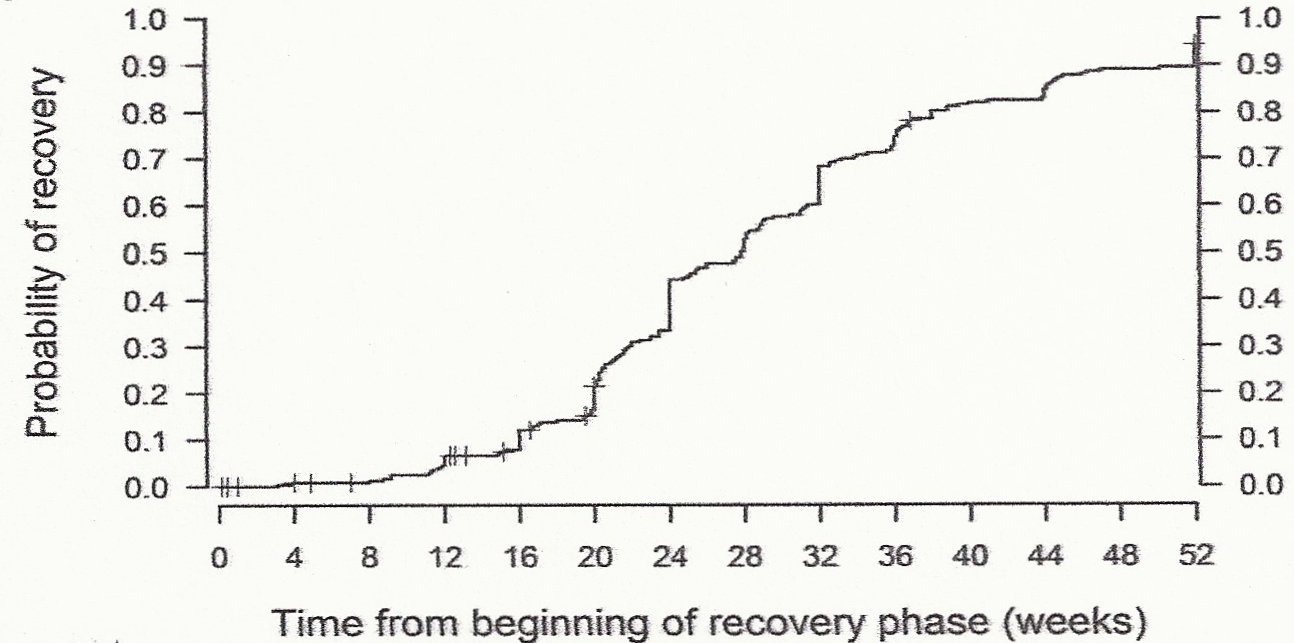
However, slower still is recovery. It took a whole year after their last injection for 95% of men to regain a nominal “recovered” sperm count, define as 15 million/mL or greater. Of the remaining 5% of men, all but one did eventually recover a count of 15 million/mL or better, but it took longer than a year. However, I note that 15 million/mL is significantly less than the average initial sperm count. In fact it is significantly less than the lowest of the group’s initial sperm counts (35 million/mL). The paper does not specify whether initial sperm count was ever regained. This might be significant as regards later attempts to start a family.
Figure 2 (Recovery defined as sperm count >15 million/mL) – click to enlarge
However, perhaps the most significant finding of the Behre et al study was that 80% of men reported that they were satisfied or very satisfied with this means of contraception and would want to continue to use it. The majority of the rest were fairly neutral, with just 5% of men being unsatisfied or very unsatisfied. Their female partners reported virtually the same levels of satisfaction. It is noteworthy that despite requiring an injection every eight weeks, and despite the minor side effects even for those not affected by the major adverse effects, 80% of men are still keen on this method of contraception. This speaks of a vast unmet need. Pharmaceutical companies please note.
But are pharmaceutical companies very interested in male contraception? With the number of initiatives that are being, or have been, pursued (e.g., see this review, and this) you might get the impression that they are keen. But this is to misunderstand the situation. It is easy enough for reputable research outfits to get hold of funding at the level of a couple of hundred thousand pounds (or dollars or euros). But there is an enormous chasm between small-scale academic studies like these and the full scale clinical trials necessary to licence a new drug. The latter requires investments of the order of several tens of millions of pounds, if not more. Companies are understandably cautious about committing such sums of money unless they have confidence in the subsequent market.
Another hormonal option which continues to be developed is MENT. This is a tradename for the not-so-snappy 7alpha-Methyl-19-Nortestosterone. The advantage of MENT is that it is applied as an implant. Actually 4 implants are necessary, but they need replacing only once a year. MENT is a synthetic androgen that resembles testosterone and hence is comparable to hormone replacement therapy, presumably with attendant risks, e.g., prostate enlargement.
Hormonal contraceptives are beset with side-effects. There are two other options: non-hormonal drugs and methods best described as “medical devices”.
Non-Hormonal Drug Methods
Examples of non-hormonal drugs include gamendazole which interferes with sperm development leading to incomplete sperms which are re-absorbed into the testes rather than being transferred into the semen. Tests on rats proved its efficacy at doses which produced no noticeable ill effects, but at the doses used these early rat tests were irreversible in a large percentage of cases. However, more recent trials on both rats and non-human primates using the variant H2-gamendazole have been claimed to be both 100% effective and 100% reversible. This research project, due to complete 2014, claimed that H2-gamendazole was “nearly ready to approach the US Food & Drug Administration for registration as an Investigational New Drug” (which essentially means “ready for clinical trials on humans” – see here). So what happened?
Another non-hormonal candidate is Phenoxybenzamine, a drug developed to lower blood pressure (an alpha-blocker). The effect of phenoxybenzamine in preventing sperm egress to the prostate, and perhaps causing a completely ‘dry orgasm’, has been known since at least 1984. However, to my untutored brain it seems an unlikely candidate as a male contraceptive given that its use in the treatment of benign prostatic hyperplasia has been discontinued due to unfavourable side effects, including tachycardia, diarrhoea, bronchoconstriction, dizziness, drowsiness and tiredness. However, researchers at King’s College London and University College London have created a prototype that is claimed to evade these problems and together, they are now seeking funding to start trials of the pill on rams.
There are also several plant-based non-hormonal candidates. Probably the most promising is Gendarussa, derived from the plant Justicia gendarussa. Tribesmen in Indonesia have long used the shrub as a contraceptive. It is hypothesised to work by preventing the head of sperm being able to penetrate the egg. Pills of Gendarussa have passed Phase II of clinical trials on humans in Indonesia. Following a third successful trial the drug could go onto the market in Indonesia. This sounds promising. To be available in the UK the pill would need to undergo more clinical trials to meet our health test standards. But if many man-years of experience accumulates in Indonesia without undue adverse indications, there will, perhaps, be an irresistible impetus to ratification in the UK ultimately.
Another plant-based product are the seeds of the carica papaya, which have been eaten by men in parts of South East Asia for many a generation. In the first study conducted on this, an extract of papaya seeds was fed to rats, resulting in decreased semen and a one hundred per cent efficacy, but with less than ideal side effects – due to the extract’s toxicity, the rats experienced dramatic weight loss. A chloroform extract of seeds tested on monkeys, however, caused low sperm production, no toxicity, no change in testosterone levels and full recovery within five months (see references linked from here or here). Similarly, a 2011 study showed that an extract of the seeds in ethanol proved 100% effective and reversible in rats. I failed to determine whether clinical trials on humans are underway, so I assume not though one source suggested otherwise.
There are several other plant based substances with potential contraceptive properties reviewed here and here. For example, the injection of minute quantities of neem oil into the vas deferens has been successfully tested as an alternative to surgical vasectomy. Successful trials of neem administered orally to rats and monkeys have been reported to result in reversible contraception. As far as I could discern, none of these other plant based compounds are front runners for development nor have any been tested under scientific conditions on humans (though men in many rural parts of India are reputed to take neem, apparently with the desired effects).
Medical Devices
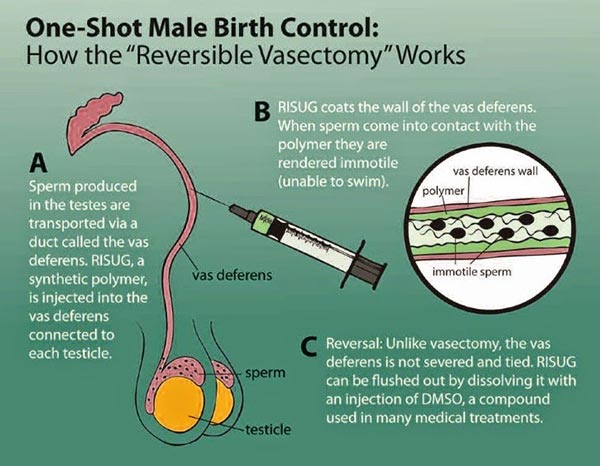
And finally we have the “medical devices”. These work by physically blocking the passage of sperm along the vasa deferentia. Consider firstly Vasalgel. This is a polymer which is injected into both the vasa deferentia. It is being developed by the Parsemus Foundation in the USA. Tests on a range of animals, including rabbits and baboons, have shown that it definitely works, for up to a year after injection (and counting). Tests show that the method is reversible in rabbits. This is accomplished by flushing the Vasalgel from the vas deferens with an injection of sodium bicarbonate (baking soda) solution. However, I believe reversibility has so far been problematic in larger animals. The Vasalgel site warns that “until reversibility studies are done in men, Vasalgel should be thought of as a vasectomy alternative“.
One source suggested that human trials of Vasalgel have been put back to 2018, though the Vasalgel site still claims that human trials will start in 2017. I’ve donated a modest sum to this one.
An advantage of Vasalgel compared with other “vas blocking” methods is that while it blocks sperm, other fluid can still pass through. This should reduce any risk of pain due to back pressure, an occasional issue with vasectomies. This could make Vasalgel a best-seller, even among men seeking a permanent contraceptive option. So Vasalgel may be a viable product even if the reversibility problem is not solved.
There is another product which is quite similar to Vasalgel, namely RISUG (Reversible Inhibition of Sperm Under Guidance). Like Vasalgel, RISUG is an injectable polymeric compound that partially blocks the vasa deferentia, providing effective contraception for up to 10 years per dose. Unlike Vasalgel, RISUG is claimed to have a spermicidal effect in addition to simple blockage.
It is claimed that implanting of RISUG, in the hanfds of a skilled practitioner, would be a 15 minute, no-scalpel, out-patient procedure. It is effective immediately, has few side effects, and has proven to be reversible in primate studies. Like Vasalgel, reversal can be accomplished using an injection of baking soda. I believe reversal has now been demonstrated in men, though the impact on the individual’s reproductive health and offspring following reversal remains a concern, along with possible carcinogenicity or mutagenicity.
This contraceptive completed Phase I and II clinical trials in India as long ago as 1997. Men who took part in the first clinical trial have had RISUG implanted for 15 years with no ill effects. No pregnancies were reported during the 3 years of the trials (nor have any been reported informally since). Phase III trials were underway in India as of 2014.
malecontraceptive.org sates that “our research has convinced us that RISUG is the most promising of the potential male contraceptives”. However, progress is glacially slow given that successful Phase II trials completed 20 years ago, and despite development being pursued in the USA since 2010 as well as India. Part of the delay is explained by this extract from malecontraceptive.org,
“In October 2002, government officials aired concerns about RISUG in India’s national press. Their concerns have since been resolved, but the controversy stalled the clinical trial for six months. The next delay was due to concerns about RISUG’s initial toxicology tests. The Indian Council for Medical Research has reviewed the toxicology data three times and approved it each time. However, in February 2002, World Health Organization scientists stated that the 25-year-old toxicology studies did not meet more recent international standards. RISUG was submitted for a new round of tests at a US lab, and approved in July 2005. In March 2006, the trial was slated to resume at 4 centers around India. Then a manufacturing delay halted progress. The pharmaceutical company making RISUG was finally able to deliver a batch produced to the World Health Organization’s Good Manufacturing Practice standards in March 2007. The trial resumed in earnest in April 2007. The trial’s data collection, analysis and publication process will take several years to complete.”
Ten years later, we’re still waiting.
Next up there are the Intra-Vas Devices (IVD). Like Vasalgel and RISUG these work by blocking the vasa deferentia. Unlike Vasalgel and RISUG, IVDs are solid devices, not deployed as injectable liquids. The US variant IVD consists of tiny, flexible silicone plugs, two of which are inserted into each vas deferens. The Chinese varaint IVD is a flexible urethane tube containing a close nylon mesh which acts as a sieve to trap sperm. This arrangement allows fluid, but not sperm, to pass through the tube, preventing the build-up of pressure that is often associated with a vasectomy. The procedure for fitting of either device is comparable to a vasectomy. This is commonly termed a “no-scalpel” procedure, but it necessarily involves making a small snip in the scrotum in order to pull out a small loop of the vas deferens (see this video). Consequently fitting an IVD can be performed as an out-patient procedure under local anesthetic in around 20 minutes. Reversal is anticipated to be almost as quick, though it is not clear to me that it has yet been done.
One of the positive features of IVDs is that they are made of materials which have already been approved for medical use, thus obviating much of the toxicology proofs. The depressing thing, though, is once again that progress always seems just around the corner. When this account was written, the author was anticipating having “European, Canadian and US approval by 2010“. Oh, yeah? But recent accounts are still telling us that “both types of IVD are currently undergoing human trials, which means they could be available within the next several years“. It’s hard not to be sceptical.
And for the grand finale, enter the Bimek SLV. The brainchild of Clemens Bimek, a German carpenter, the Bimek SLV is a switchable valve. The plan is to insert one of these devices into each vas deferens. The switch can be felt and pressed through the scrotum, thus closing the valve and preventing sperm getting passed (watch the video). Want a baby? Just flick the switch back again (there is a safety catch to prevent accidental opening of the valve). It is elegant simplicity itself. The device is 11 x 18mm though, so fitting it will be a more significant surgical procedure than fitting an IVD. However, no further operation is needed to reverse your contraception – which is a very big plus. Also – and I feel rather guilty for mentioning this – you could choose to be fertile with one woman and infertile with another.
And the snag? Well, guess what? Herr Bimek just needs your money to pay for the clinical trials. Sound familiar? And despite the media coverage Bimek SLV received in 2016, Clemens Bimek’s web site has fewer than 3000 supporters as I write – and I guess very few have handed over cash.
And like every other male contraception, Bimek SLV has a longer history than you would think – because the popular press always presents these ‘stories’ as something brand new, ignoring the long past history. Herr Bimek had one of his devices fitted himself back in 2009, and an upgrade fitted in 2012. In January 2016, Bimek was the only man to have had one of his devices fitted. Is he still? He was looking for 25 volunteers. I wonder how successful he was in finding them?
I also wonder if Herr Bimek has the faintest clue about how to conduct a clinical trial that will impress the State controlled authorities which stand poised to crush his endeavors merely for having the presumption to make the attempt?
I apologise if it seems I am being hard on Clemens Bimek. In truth I suspect his idea is a very good one, and there is no technical reason why it should not do well. The device is good, and there is a ready market. Surely the two together make a winning hand? Ah, in the Victorian era, maybe. But not now, Herr Bimek, not now. These days you must cross the Valley of Death, the chasm which comprises clinic trials plus nameless and faceless Committee members with power of veto over anything and an agenda which none know. I guess Bimek is one of those honest individuals, too innocent to appreciate what barriers lie ahead. I wish him the best of luck. Sometimes the holy fool does triumph.
The Social and Economic Environment
But let me end on a more sober note. What demand is there, exactly? A study published in Human Reproduction 20, 2, 549–556 (2005) indicated that around half of men would be open to using a male contraceptive. The on-line survey in this Telegraph article suggests 81% of responders to the question “would you take the male pill?” said yes.
The first meeting of the International Consortium for Male Contraception held in Paris in May 2016 came up with a Paris Manifesto: It’s Time for New Male Contraceptives. Depressingly, it was no more ambitious than this: “Our goal is to help bring to market at least one reliable, reversible and affordable male contraceptive by 2026“. Still, if 2026 was guaranteed, I’d go for it. It isn’t.
The problem is money. Aaron Hamlin, Executive director of the Male Contraception Initiative, says, “Funding is tough. In fact, there’s more money dedicated to figuring out how best to sterilise your family pet than there is to researching new male contraceptives“.
One of the negative factors is the perception by the pharmaceutical companies that sales of a male contraceptive may simply be offset by reductions in sales of female contraceptive. Personally I suspect this is a largely false perception. Whilst there is bound to be such an effect, I suspect the new market in male contraception would vastly exceed the small decrease in female contraception. This is pretty obvious when people not within a stable partnership are considered – and that’s a large market on its own.
The non-drug based “medical device” options offer a potentially far easier route to licensing. For this reason my money would be on those methods (literally in one case).
The USA National Institutes of Health spent $424M on this area in 2015, but much of that goes to research in female contraception and reproduction. You might think they could run to funding clinical trials on male contraceptives. But there is no political will to do so. States are not too keen on the prospect of population collapse – which is precisely why male contraception would be a potent weapon for men to wield against the State. But for that reason we cannot look to the State for funding. The pharmaceutical companies need to be persuaded that they stand to gain megabucks by backing male contraception. I believe they do. It’s our job to press the case.
It is worth recalling the history of the development of the female Pill. Although development of The Pill was the work of Gregory Pincus and John Rock, their work was privately funded by a rich woman: Katharine McCormick. McCormick was a suffragist and a women’s rights activist. She obtained her wealth by marrying a rich man and was happy to use it to fund a genuine need for women to be able to control pregnancy. McCormick’s involvement with The Pill was facilitated by Margaret Sanger, birth control pioneer and first-wave feminist. All told, in today’s money, McCormick provided tens of millions of dollars – almost all the funding required. The Pill eventually gained a licence for contraceptive use in the USA in 1960 (by which time McCormick was 85). The rest is history, as they say – but actually it is the story prior to this which is the history. The message here is that it was the women’s lobby, what we would now call first wave feminists, who funded the development of The Pill. Men’s activists today should be directing rich men’s attention to the equivalent endeavours on behalf of men.
The reason why we do not have a male contraceptive already is not technological: it is money and political will which is lacking.
Pingback: Male Contraception Initiative | The Illustrated Empathy Gap
“The pharmaceutical companies need to be persuaded that they stand to gain megabucks by backing male contraception”
—————————-
Let me get this straight.
You think that they need PERSUADING?
You think pharma isn’t at least half run by hetero men (who therefore know exactly what it’s like to be a young hetero man)?
You think that sexually active men wouldn’t use a viable, ubiquitous ‘male pill’?
Either a male ‘pill’ (of any shape or form) isn’t viable OR it’s being actively suppressed.
Considering all the methods described in this article do you really think a male pill of some kind isn’t viable?
So what does your common sense suggest is the more likely possibility?
And what does common sense suggest is most likely at the bottom of that suppression?
If you say feminists you may be only partially correct.
Does a woman need necessarily identify as a feminist to be (secretly) against a male pill?
Very few people would not agree that the Pill changed society in many core ways. The male Pill has the same potential as men regain control of some of their reproductive rights, of which they have almost zero at this time.
Interestingly, I think that it would not be primarily mostly men who would take advantage of the new male Pill, but what I envisage is millions of mothers taking their teenage sons to the clinic to have the Pill.
There would be a huge effect on national populations of course, but I believe that would be insignificant compared to the societal changes – mostly for the benefit of men.
Another great article by William. Thank you for the careful research and the ongoing effort to educate us all about men’s rights and lack thereof.
Hopefully the reasoned arguments and careful scholarship will convince more men to be become active in trying to restore true equality for both men and women.
Joseph