
Oh really? You must forgive me if I am less than impressed by the much vaunted female capacity for empathy. It appears to be rather partisan in its application.
Our society condones chopping body parts off babies for no medical reason – as long as they are boy babies.
Read that again. It is not an exaggeration. Nor is it rare.
Not only is the process of male genital mutilation (MGM) abhorrent, the result can be very harmful for the adult male, throughout his life. The purpose of MGM is to ameliorate male sexual function. It does, though those mutilated as babies will have no basis for comparison.
I realise that many circumcised men are content with their condition. But a great many are not. I also realise that many circumcised men will be sensitive about their condition and may not welcome it being referred to as mutilation. I understand and am sympathetic to this, but a reluctance to be forthright about the issue is surely part of the problem.
How is MGM carried out?
The mutilation may be done by surgeons or by traditional practitioners. It may be carried out on babies or boys or adult men. Where the individual is old enough to elect freely to be circumcised I have no issue with it. Your body, your choice. My concern is with the practice of circumcising infants or boys too young to give meaningful consent. My concern extends to cases where, even though the individual may be sufficiently mature to give consent, this consent cannot be regarded as freely given due to a virtually obligatory cultural expectation.
You can find videos of circumcisions carried out as surgical procedures in the west here (not for the squeamish). I believe this is still the method most often employed in the USA, where more than half of boys are still circumcised as new babies even today. There are many different types of clamp used in the surgical procedure in which the foreskin is cut off by scalpel. In the UK I believe the most common method used by doctors now is the Plastibel device, but there are others in common usage in the USA.
For older boys, or adult men, an alternative is an ERCD (Elastic Radial Compression Device). These devices cause necrosis of the foreskin over a period of time by starving it of blood flow due to radial compression applied by an elastic ring. Imagine tying a tight ligature around the base of your finger until it turned black and fell off. That’s about it. I exaggerate, of course. A finger contains a bone whereas the foreskin does not. Nevertheless, you get the picture.
Traditional circumcisions come in a variety of forms. You probably believe that male circumcision is legal in the UK (and, indeed, almost everywhere). But you may not have realised that male circumcision is also unregulated. Anyone can do it. You or your local barber can set yourselves up as circumcisers. Some amateur practitioners in the UK may use ordinary household scissors, some olive oil and cotton wool. No anaesthetic is involved, obviously. Jewish Mohels have their own methodology, and associated ceremony (brit milah), which includes some distinctly unhygienic practices.
Actually I now believe that male circumcision is illegal in the UK. The practice is tolerated rather than legal. There is a credible legal case that male circumcision constitutes the offence of actual bodily harm or possibly grievous bodily harm. That MGM is not currently prosecuted rests precariously on a single throw-away remark by one judge based on no legal argument whatsoever, and apparently made merely to conform with the status quo. In effect, the criminal justice system, the police, the crown prosecution service and the judiciary, are failing to implement the law. Most likely this is to avoid upsetting religious groups – though this is a peculiar situation in countries where the majority of those circumcised are not subject to this procedure for religious reasons, e.g., in the USA, Canada and Australia. The Germans got close to a ban in 2012, but then backed-off, see here and here.
Someone explain this to me. If I cut off a baby’s ear or finger, I would rightly find myself prosecuted for grievous bodily harm and probably imprisoned. It is even illegal to tattoo a child in the UK. But in the special case of a male baby’s foreskin, it’s OK. Cut away. What? What?
You may be reticent about setting up as an amateur slicer of the penis. After all, in the USA more than 100 babies die each year from circumcisions. But perhaps you need not worry. In 2010 the ironically named Goodluck Caubergs bled to death at 27 days old after suffering the ministrations of Manchester midwife Grace Adeyele. She was subsequently convicted of homicide but received only a suspended sentence.
To encourage you further into the business of circumcision, in 2012 when one month old Angelo Ofori-Mintah died from massive blood loss two days after being circumcised at home by a Mohel, the Rabbi faced no charges. A verdict of accidental death was returned.
Ally Fogg has told us that in Rusholme, Manchester, there is a notice on a first floor window offering circumcisions, quite literally in a backstreet above a kebab shop. The same source informs us that in one Manchester hospital alone there are three cases of bleeding circumcisions per month, any one of which could be another Goodluck Caubergs were it not for medical intervention. And in just one Birmingham hospital in one year, 105 boy babies were treated for complications arising from circumcision, about one per month being life threatening.
But all this pales into insignificance compared to the horror story that is traditional circumcision in Africa.
From the South African Health News Service we learn that between 2008 and 2014 nearly half a million young men have been hospitalised in the Eastern Cape and Limpopo districts alone. The data comes from a report from the Commission for the Promotion and Protection of the Rights of Cultural, Religious and Linguistic Communities (CRL). Based on community consultations, the report also highlighted that at least 419 boys had died in the two provinces during the same period. Over 900 boys have died in the Eastern cape alone over the last 20 years. Scale this up, if you will, to the whole of Africa.
Many hundreds of boys are permanently maimed annually in the Eastern cape alone. Dr Dingeman Rijken’s site includes photographs showing just what “maiming” means. You will need a strong stomach.
If I had my way, the woman whose picture heads this post would be reincarnated as one of these boys. No doubt she would enjoy the male privilege of being able to ‘make choices about her own body’, free from culturally imposed expectations.
Who is mutilated?
Do not make the mistake of thinking that MGM is purely a religious issue, affecting just Jews and Moslems. In all Anglophone countries the majority of the mutilated are not Jewish or Moslem. In the UK about 18% of adult males are circumcised compared with about 5% who are Jewish or Muslim. Circumcision is reputed to be more common amongst the highest socioeconomic classes. British royalty has a tradition of circumcising its male members (sorry), probably as a hang-over from the Victorian era (see below).
The highest incidence of MGM in Anglophone countries is in the USA where the rate of infant circumcision is at least ~56%, and higher in some states. The percentage of males in the USA who have been circumcised is greater than this due to falling rates after Medicaid funding was withdrawn for the procedure in many States. This huge prevalence of MGM compares with just 2.7% of the US population being Jewish or Muslim.
In Canada, 32% of men are circumcised compared with 4% being Jewish or Muslim.
In Australia, infant circumcision rates have reduced substantially but are still running at perhaps around 14%. However a 2005 survey found that the prevalence of MGM in Australia was then roughy 58%. These figures compare with only 2.2% of the population being Jewish or Muslim.
(Sources of the above data here and here).
Hence the overwhelming majority of victims of MGM in Anglophone countries are not circumcised for religious reasons. (Worldwide, however, Islam would account for the majority of circumcisions).
Personal testimonies
The links below are to videos. They are strongly recommended viewing. The first two are the personal testimonies of circumcised men of some standing. The second two are scientific studies showing how very damaging is foreskin removal.
John Warren is a UK doctor and the founder of NORM-UK. He talks here about his intactivism
Ken McGrath describes the anatomy and histology of the foreskin, and provides comprehensive scientific evidence that the skin that is removed in circumcision is the most sensitive part of the penis – in fact of the whole body.
George Denniston, MD, of Doctors Opposing Circumcision. He reminds us that there is no national medical society in the world that recommends routine infant circumcision.
The claimed benefits
So, if it is not for religious reasons, why is male genital mutilation carried out?
It’s hygienic, don’t you know. The foreskin can harbour germs.
Hmm. Not heard of soap and water then? The penis is very ease to clean. Easier, than, say, cleaning under your finger nails. Ah! I have a great idea. I can solve my finger nail cleaning problems by chopping my fingers off. Doesn’t really stand scrutiny, does it? The vagina presents a significantly greater challenge as regards hygiene, simply for anatomical reasons, but no one would use this as a justification for female genital mutilation. That would be hateful. Yes, it would.
Claims that MGM has medical benefits are merely paper-thin, fallacious post-hoc rationalisations (or bollocks, in short).
Prior to the Victorian era, circumcision was uncommon in Christian Britain. It became popular in the Victorian era because it was claimed to be a cure for that most dreaded moral degeneracy, masturbation. The Victorians had a thing about Onanism. A couple of quotes convey the prevailing ‘wisdom’,
It (self abuse) lays the foundation for consumption, paralysis and heart disease. It weakens the memory, makes a boy careless, negligent and listless. It even makes many lose their minds; others, when grown, commit suicide…. Don’t think it does no harm to your boy because he does not suffer now, for the effects of this vice come on so slowly that the victim is often very near death before you realize that he has done himself harm. It is worthy of note that many eminent physicians now advocate the custom of circumcision… (Mary R. Melendy, MD, The Ideal Woman – For Maidens, Wives and Mothers, 1903).
A remedy for masturbation which is almost always successful in small boys is circumcision. The operation should be performed by a surgeon without administering an anaesthetic, as the brief pain attending the operation will have a salutary effect upon the mind, especially if it be connected with the idea of punishment. In females, the author has found the application of pure carbolic acid to the clitoris an excellent means of allaying the abnormal excitement. (John Harvey Kellogg, M.D., “Treatment for Self-Abuse and its Effects,” Plain Fact for Old and Young. Burlington, Iowa: F. Segner & Co. (1888). P. 295)
Hmm, I don’t think much of his corn flakes either. These quotes would be funny if they had not had such serious consequences.
But it was not only masturbation which they claimed could be cured by circumcision. No, there is hardly a disease known to man that has not at some time been claimed to be cured by MGM – see, for example, this video. (Strongly recommended, but the data for the UK after 1950 is rather an under-estimate. Look out for the researchers called Cockshut and DeCock, I kid you not).
The WHO and HIV
The latest in this long line of diseases that MGM can prevent is AIDS, so some claim. The evidence supporting the contention comes from just three randomised controlled trials, the latest being that of Bailey, et al, The Lancet 369 (9562): 643–656, February 2007. It claimed an incidence of HIV in a circumcised group smaller than that in a control group by about a factor of two.
These studies have come in for severe criticism on methodological grounds, largely because the monitoring boards terminated the most recent pair of studies prematurely. For example, Mills and Siegfried, The Lancet 368 (9543): 1236, concluded that “The circumcision trial is …at risk of serious effect overestimation. We therefore advocate an impartial meta-analysis of individual patients’ data from this and other trials underway before further feasibility studies are done“.
Nevertheless, largely on the strength of the study of Bailey et al, the World Health Organisation (WHO) and the Joint United Nations Programme on HIV/AIDS (UNAIDS) have recommended that male circumcision is an efficacious intervention for HIV prevention.
I find it staggering that the WHO can blithely recommend wholesale mutilation of entire populations. But they are doing so. In 2011 the WHO’s plan was to circumcise 20 million men by 2015 in 14 nations in Sub-Saharan Africa. Are men humans or cattle? Below I shall take a closer look at one of these countries, Rwanda.
The WHO/UNAIDS recommendation has come in for severe criticism. For example, Dowsett and Couch, Reproductive Health Matters 2007;15(29):33–44, are far from convinced that enough evidence exists to motivate wholesale circumcision as an HIV preventative. They are far from alone. Eight studies which contra-indicate any benefit of circumcision, or actually indicate a disbenefit, are listed in my earlier review. The vlogger 5hadowfax has produced an excellent video summarising the fatal shortcomings of the trials upon which the WHO/UNAIDS recommendation is based.
A more recent refutation of the WHO position has come from South Africa. In reply to the Co-Director of NOCIRC-SA (National Organisation of Circumcision Information Resource Centres, South Africa) on 23 June 2011, the South African Medical Association wrote the following letter,
CIRCUMCISION OF BABIES FOR PROPOSED HIV PREVENTION: The matter was discussed by the members of the Human Rights, Law & Ethics Committee at their previous meeting and they agreed with the content of the letter by NOCIRC SA. The Committee stated that it was unethical and illegal to perform circumcision on infant boys in this instance. In particular, the Committee expressed serious concern that not enough scientifically-based evidence was available to confirm that circumcisions prevented HIV contraction and that the public at large was influenced by incorrect and misrepresented information. The Committee reiterated its view that it did not support circumcision to prevent HIV transmission.
In passing I note that even if one believes that male circumcision is efficacious against HIV, the proffered mechanism involves “the susceptibility to HIV in Langerhans cells in the inner foreskin, and a protective keratinisation that occurs after circumcision.” (Dowsett and Couch, Reproductive Health Matters 2007;15(29):33–44). They go on to note that Langerhans cells occur in the clitoris and the labia and other parts of female genitalia but no one is talking of mass genital mutilation of females in the name of HIV prevention. Of course not. That would be hateful. Yes, it would.
Medical rejection of the claimed benefits and recognition of the harm
Authoritative medical bodies around the world have come out against any general medical benefit from circumcision. For example,
- The Royal Australasian College of Physicians (2010): “After reviewing the currently available evidence, the RACP believes that the frequency of diseases modifiable by circumcision, the level of protection offered by circumcision and the complication rates of circumcision, do not warrant routine infant circumcision in Australia and New Zealand.”
- The RACP, Australian Association of Paediatric Surgeons, New Zealand Society of Paediatric Surgeons, Urological Society of Australasia, Royal Australasian College of Surgeons, and Paediatric Society of New Zealand have corroborated the Canadian Paediatric Society (2004), declaring that circumcision of newborn males should not be routinely performed. The statement firmly declares: “There are no medical indications for routine male circumcision.”
- Canadian Paediatric Society (1996): “The overall evidence of the benefits and harms of circumcision is so evenly balanced that it does not support recommending circumcision as a routine procedure for newborns.” Note that the cost-benefit analysis in this Canadian report ignored diminished sexual function, probably the most serious effect of circumcision.
- The Central Union for Child Welfare, Finland (2003): “Circumcision of boys that violates the personal integrity of the boys is not acceptable unless it is done for medical reasons to treat an illness. The basis for the measures of a society must be an unconditional respect for the bodily integrity of an under-aged person. Circumcision intervenes in the sexual integrity of a male child causing a permanent change in organs and has consequences pertaining to both health and quality of life. The circumcision of girls is rightly considered as inhuman mutilation of the genitals and is punished abuse. Also boys must be guaranteed a similar protection by law. According to the opinion of the Central Union for Child Welfare in Finland nobody has the right, on behalf of the child, to consent to operation, violating the bodily integrity of the child, if it is not done to treat an illness.“
- The Royal Dutch Medical Society (2010): “There is no convincing evidence that circumcision is useful or necessary in terms of prevention or hygiene. Partly in the light of the complications which can arise during or after circumcision, circumcision is not justifiable except on medical/therapeutic grounds. Non-therapeutic circumcision of male minors is contrary to the rule that minors may only be exposed to medical treatments if illness or abnormalities are present, or if it can be convincingly demonstrated that the medical intervention is in the interest of the child, as in the case of vaccinations. Non-therapeutic circumcision of male minors conflicts with the child’s right to autonomy and physical integrity. There are good reasons for a legal prohibition of non-therapeutic circumcision of male minors, as exists for female genital mutilation.”
- British Medical Association (2006): “In the past, circumcision of boys has been considered to be either medically or socially beneficial or, at least, neutral. The general perception has been that no significant harm was caused to the child and therefore with appropriate consent it could be carried out. The medical benefits previously claimed, however, have not been convincingly proven, and it is now widely accepted, including by the BMA, that this surgical procedure has medical and psychological risks. It is essential that doctors perform male circumcision only where this is demonstrably in the best interests of the child.”
- The British Association of Paediatric Surgeons advises that “there is rarely a clinical indication for circumcision.”
- American Academy of Family Physicians (2002) emphasizes the lack of therapeutic benefit and likens neonatal circumcision to a “cosmetic” procedure and expresses ethical concerns about non-therapeutic neonatal circumcision.
- The American Medical Association (1999) has called for the re-training of American physicians and improved information to parents in hopes of reducing the unacceptably high rate of non-therapeutic neonatal circumcision.
- United Nations Convention on the Rights of the Child (1989) states that children have a right to grow up free of traditional practices that are prejudicial to health.
- Doctors Opposing Circumcision web site states, The claims of “potential benefits”, allegedly provided by medically unnecessary, non-therapeutic circumcision, lack any real support from medical science…..Removal of the nerves of the foreskin by circumcision produces a deficit in sensory input into the central, parasympathetic, and sympathetic nervous systems. One, therefore, would expect to find alteration in sexual response. Several recent studies have found this to be the case.
The real reason for MGM
This is how Moses Maimonides, the Jewish intellectual and physician, expressed it as early as the twelfth century,
“With regard to circumcision, one of the reasons for it is, in my opinion, the wish to bring about a decrease in sexual intercourse and a weakening of the organ in question, so that this activity be diminished and the organ be in as quiet a state as possible. It has been thought that circumcision perfects what is defective congenitally…How can natural things be defective so that they need to be perfected from the outside, all the more because we know how useful the foreskin is to that member? In fact this commandment has not been prescribed with a view to perfecting what is defective congenitally, but to perfecting what is defective morally. The bodily pain caused to that member is the real purpose of circumcision. None of the activities necessary for the preservation of the individual is harmed thereby, nor is procreation rendered impossible, but violent concupiscence and lust that goes beyond what is needed are diminished. The fact that circumcision weakens the faculty of sexual excitement and sometimes perhaps diminishes the pleasure is indubitable. For if at birth this member has been made to bleed and has had its covering taken away from it, it must indubitably be weakened. In my opinion, this is the strongest of the reasons for circumcision. Jewish men, sexually subdued and readily controlled by their wives, don’t stray into mischief. The power of his member has been diminished so that he has no strength to lie with many lewd women.”
No one has said it more clearly. The purpose of MGM is to diminish male sexual function.
We have already noted its role in frustrating masturbation (though it does not prevent the determined). And we shall see below that reduction of sensitivity is the defining characteristic of the circumcised penis, even to the point that some men report giving up sex altogether.
As always we must ask cui bono – who benefits from a reduction in the dreaded male sexuality? Moses Maimonides has told us. It is a form of control which society exercises on men.
The harm done
I have already given some examples above of what can happen if circumcision is botched, including death or complete loss of the penis. But what if the operation itself goes as planned. What harm does a well executed circumcision inflict? Some of the most common complaints of circumcised men from the on-line survey here were as follows: insensitive glans (67%); dry, keratinized glans, needs lubricants before sex (75%); excess stimulation needed to achieve orgasm (59%).
There is an excellent video summarising the results of the 2012 Circumcision Harm Survey.
Other comments left by the respondents included: Wooden stick feeling during sex; Scar is too tight to accommodate a full erection comfortably; Glans is sensitive but in a sandpaper sort of way, not pleasurable; Complete sexual dysfunction with no feeling whatever; No pleasure and feeling of envy towards intact boys; Penis bent on erection, will not straighten (this is a well known syndrome resulting from circumcision); If I wear a condom I feel absolutely nothing.
In answer to how they felt about their condition, the responses were: Anger (71%); Frustration (72%); Betrayed by mother/father/doctor for lack of protection (55% / 50% / 58%); Dissatisfied with my condition (77%); Mutilated (61%); Violated (55%); My human rights were violated (73%).
Scientific tests have confirmed that, not only does circumcision reduce the sensitivity of the glans, but the foreskin, the very tissue which is removed, is the most sensitive of all (see this video).
Rwanda – A Case Study
Rwanda has taken seriously the WHO’s recommendation to implement MGM as an HIV preventative. Nearly three years ago they started a programme of circumcising 700,000 men between the ages of 15 and 50. They were aiming to achieve this goal in 2016. The ultimate aim is to circumcise 2 million men.
But a couple of hours Googling was enough to convince me that even circumcising the entire male population will do no good. One simply needs to look across all African nations at the prevalence of HIV against the percentage of the population circumcised.
I took data for the prevalence of HIV by country from WHO/UNICEF, here and here and here (data from 2013 or earlier, so prior to the Rwandan MGM initiative). Data for the percentage of males circumcised by African country was taken from Williams et al. (2006), “The potential impact of male circumcision on HIV in sub-Saharan Africa“, PLos Med 3 (7) 262. The result is Figure 1 below.
Figure 1: % HIV versus % Circumcision in Africa (2013)
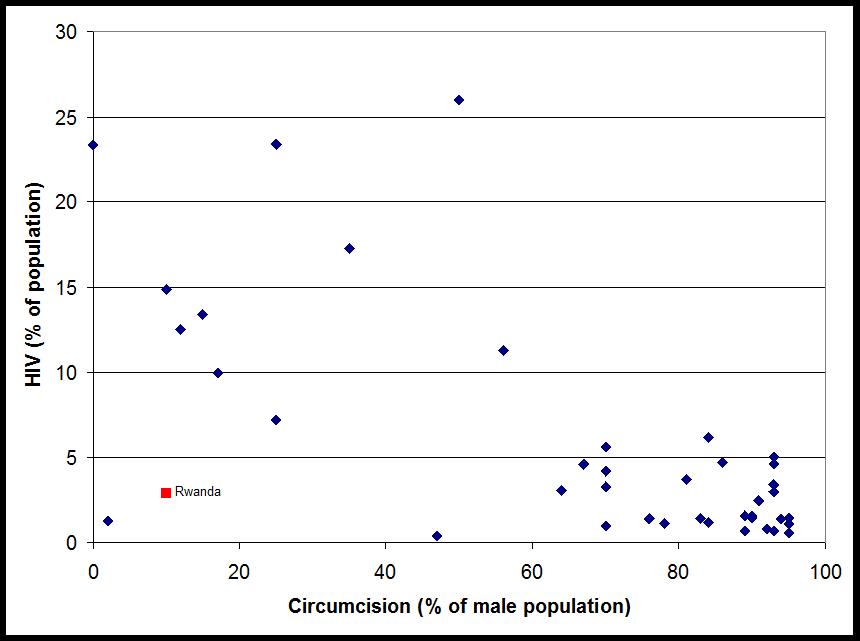
It is true that the incidence of AIDS is greatest in countries with low rates of circumcision. But we all know that correlation is not causality. For example, the high rates of circumcision may be related to countries with dominant numbers of Moslems, and hence low alcohol consumption. The significant factor might be alcohol consumption. I’m not claiming this is so. It is just an illustration of the danger of assuming correlation is causal.
However, even if Figure 1 does identify a genuine causal link between MGM and lower HIV incidence – look where Rwanda lies. Despite having only a small proportion of circumcised men (~10% in 2013) it also had, at that time, a relatively small HIV incidence for an African country (2.9%).
Now look at the HIV incidence in African countries which have over 90% circumcised men. The spread is between a fraction of one percent and ~5%. The average HIV rate for African countries with circumcision rates greater than 60% is 2.6%, virtually the same as that of Rwanda.
Given this observation, even knowing nothing whatsoever about the epidemiology of HIV, what chance is there that the mass mutilations of Rwandan men will have any beneficial effect? Very little, I suggest.
It may make matters worse. It is certain that condom usage is far more beneficial than circumcision as regards preventing HIV infection. So if being circumcised were to lead to reduced condom usage, as it well might, then HIV incidence could feasibly increase. Time will tell.
The Feminist Position
The feminist stance on MGM is well illustrated by the Guardian. The newspaper frequently runs campaigns against FGM. But if you leave a comment after such an article along the lines, “I agree that FGM is an abomination and should be stamped out, but why do you never speak out against MGM?” the Guardian’s moderator will remove the comment. I speak from experience. It matters not how gently worded it may be. Recently the Guardian has admitted that they have a policy of removing all comments relating to MGM. But, hey, feminism is about equality and feminism is for men too.
Worse, women’s groups will actively oppose moves to outlaw MGM on the grounds that “it would have the effect of putting male and female circumcision on the same footing, when they were in no way comparable“. Such a stance may be mocked by noting that it is equivalent to regarding chopping someone’s finger off as acceptable because it is not as bad as chopping off an arm. But the feminist stance does not arise from lack of logic. It arises from lack of compassion and from a cold blooded, partisan ideology. The motive power behind feminism is the imposition of a narrative of female victimhood and male power. No instance of male victimhood must be allowed to surface in the public mind, or the feminist charade may be exposed.
Incidentally, it is not necessarily the case that FGM is worse than MGM. Both exist in a variety of degrees of severity. A rational comparison is made in this video.
We live in a society in which you may be imprisoned for fondling a woman’s breast but in which cutting off part of a boy’s penis without his consent is acceptable, even encouraged. And yet the indestructible public perception is of female disadvantage and male privilege.
The most disturbing evidence I have yet seen that feminist male-hatred may be playing a part in MGM is this extremely nasty female paediatrician. Why has this woman not been struck off?
For further reading see, for example, Brian D Earp’s blog.
Addenda
(Added 1/1/17): Tribal circumcision ritual becomes Africa’s latest tourist attraction – The Ugandan Government and Uganda Tourism Board now hopes to attract international visitors. Attendance fees are being considered to help build a cultural centre celebrating and preserving the tribe’s history.
(Added 11/7/17): Just occasionally I have an outburst of optimism. Tip of the hat to the Daily Mail for publishing these pictures.